Vladimir Nesterov
Full member of Academy of Medical and Technical Sciences, Academician,
President of International Academy of non-linear diagnostic systems.
An ever-growing number of physicians enjoy an opportunity of a screening NLS diagnostics of prostate gland and urinary bladder.
This paper attempts to consider some particulars of morphological changes occurring in a prostate affected by pathology, based on the results of NLS-investigations. During research we used “Metatron”-4025M device with 4.9 GHz generator frequency.
To enhance the quality of prostate diseases diagnostics it is important to comprehend the specifics of topographic and zonal anatomy of a particular organ.
The prostate gland is located in the small pelvis between the bladder and anterior abdominal wall, anterior rectum wall and secondary urogenital diaphragm. The gland has a chestnut shape and tightly envelops the bladder cervix and prostatic urethra. The gland base is tightly connected with the bladder into a coherent mass. Its anterior surface is directed to the symphysis, and the posterior one – to the rectum ampulla. The posterior surface of the gland has an expressed sulcus, which allows to conventionally subdivide the gland into the left and right lobes. Besides, there is a protruding middle coneshaped lobe confined anteriorly by the prostatic urethra and by the spermatic ducts posteriorly.
According to zonal anatomy theory, usually four glandular zones are distinguished in the prostate. The correct interpretation of NLS data largely depends on the knowledge of their topical pattern. 20% of the glandular tissue correspond to the central zone (CZ). The peripheral zone (PZ) occupies 75%. The intermediate (transitory) zones (TZ) make up 5% of the total amount of the glandular tissue.
Perurethral glands (PUG) take a relatively small amount of the tissue, however exactly this area of the gland is very important for explaining the changes at a benign hyperplasia. Apart from the glandular area, 4 fibro muscular zones can be singled out:
1) Anterior fibro muscular stoma (AFS).
2) Unstriated muscular fibers of the urethra (UMFU).
3) Preprostatic sphincter (PPS), which is an extension of the musculature of the inferior part of the urcter and prevents inverse emission of seminal fluid.
4) Postprostatic sphincter (PPS), which is responsible for retaining urine in the bladder and blocks incontinent micturition.
The gland can be conventionally subdivided into two parts:
– external part consisting of CZ, PZ, TZ and
– internal part comprising AFS, PPS and PoPS.
According to NLS-investigation, the external part looks like a structure of normal chromogenic density (2-3 points on Flandler’s scale), and the internal one is hypochromogenic (1-2 points). A fibro muscular layer, the so-called surgical capsule, along which an incision is made during surgical intervention, and calcium salts deposit (calcium incrustation of the gland), divides the two parts. In the NLS investigation, those formations can well be seen as achromogenic structures (0 points) of different size.
If any pathological changes are detected in the NLS-graph it is recommnded to:
– specify their exact location,
– perform histography of the pathological area and area of the tissue with a normal structure.
It will be helpful for the case follow-ups. At a benign hyperplasia NLS allows to detect the direction of the principal germination. In case of hypertrophic transitory zones the gland proliferates inwards. Though “lateral chromogenic zones” are formed (4-5 points on Flandler’s scale), the nodes can still be always visualized. Threedimensional (3D) NLS offers the most detailed and authentic information.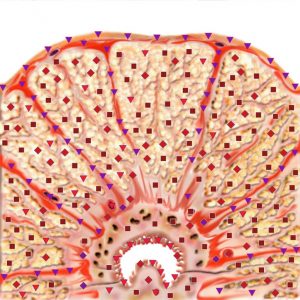
Enlarged lateral lobes squeeze PZ and CZ causing their atrophy. With proliferation of the paraurethral zones, a massive fibro muscular PPS layer restricts their hyperplasia, so with this kind of pathology the gland proliferates along the urethra forming a “middle zone of chromogenity” pushing back the bladder wall. Virtual scanning makes this pathology clearly visible in longitudinal sections.
In case of a squeezed cervix of the bladder an NLS-graph allows to visualize signs of an infravesical obstruction, that causes some morphological and functional changes in the lower and upper urinary tracts. Specifically, in the initial phases of benign hyperplasia, changes in the bladder can be observed. It happens because of compensatory hypertrophy of the detrusor.
These 3 phases of benign hyperplasia of the prostate can be distinguished, depending on the intensity of the changes:
– hyperchromogenic density of the gland;
– the above-mentioned plus dilatation of the upper urinary tract with the cortical layer of kidneys involved in the process.
Diagnosis of acute prostatitis is made on the basis of histograms (similarity to the etalon standard process “prostatitis” D<0.425).
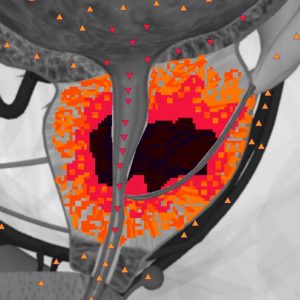
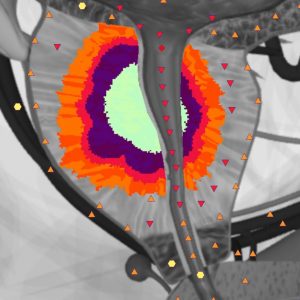
In the case of abscessed lesion, a still higher hyperchromous area (6 points) is visible against the general moderate chromogenety (4-5 points according to Flandler’s scale). Areas of frank hyperchromic changes correspond to necrotic changes. With an abscess in progress, one can notice a reduced infiltration of the tissue around the cavity with gradual decreasing of chromogenity (down to 0 points) in the course of dynamic observation. With adequate therapy applied, the postinflammatory cyst may fall into regression.
As can be seen from NLS-investigation, chronic prostatitis does not give a common characteristic picture, however the morphological processes in different phases of the disease are reflected in histograms. With a long-lasting disease the chromogenic density tends to rise due to a postinflammatory substitution for the glandular component and in histograms, in the ‘organopreparations’ mode destructuring of the fibrous component starts to predominate.
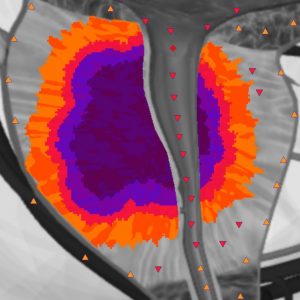
The minimum size of tumor determinable by means of NLS-investigation is about 8-10 mm. 80% of the tumorous nodes are represented by markedly hyperchromogenic proliferative structures (4 – 6 points on Flandler’s scale).
Analysis of histograms of the nidi helps differentiate an oncoprocess. The method’s sensitivity becomes higher with both “entropic analysis” and “NLS-analysis” modes in use.
Considering the fact that cancer often develops with some diffuse changes occurring on the background, for example, with chronic prostatitis or adenomatosis, it is not always possible to visualize newly formed cancerous areas. In such cases, the results of PSA level definition should be considered. The PSA level is defined considering the patient’s age and gland volume.
Therefore, NLS-method allows to diagnose most prostate diseases and being a screening diagnostics method, it should be supplemented by biopsy, should any pathological changes be detected.