Mitter S., Lehnhardt K., Elvins A
Hospital Erasme Universite Libre de Bruxelles
In order to evaluate informativity of a three-dimensional NLS-graphy in diagnostics of a pseudo-tumor-like pancreatitis, we carried out a retrospective analysis of clinical records of 328 patients admitted to the Erasme academic hospital in 2010-2011. The patients suffered from a hepatopancreatobiliary system organs pathologies complicated by a biliary obstruction; these patients formed a main group. A control group consisted of 30 patients treated in a hospital who had no pathologies of a gastrointestinal tract and a hepatopancreatobiliary system; the main group consisted of 30 patients with diagnosed chronic pseudo-tumor-like pancreatitis. We carried out a comparative analysis of a two-dimensional and a three-dimensional NLS-graphy in revealing of a chronic pseudo-tumor-like pancreatitis signs; evaluated informativity of a two-dimensional and a three-dimensional NLS-graphy and a multi-layer spiral CT in diagnostics of a chronic pseudo-tumor-like pancreatitis.
Introduction
Timely and accurate diagnostics of pancreatic diseases, without which efficient treatment is not possible, is one of the main goals of a modern gastroenterology. It is determined by increasing of disease incidence and difficulties in a differential diagnostics due to absence of pathognomonic clinical symptoms, especially in the early stages of an illness. The difficult is differential diagnostics between pancreas head cancer and a chronic pseudo-tumor-like pancreatitis that sometimes result in complications requiring surgical interventions. These diseases may look like stomach and duodenum ulcer, pylorus stenosis and be accompanied by gastrointestinal hemmorhage and acute pain in superior parts of stomach. Chronic pancreatitis is diagnosed in 0.2-6.8% of adults. It is diagnosed in 6-8% of all digestive organs diseases. Examination of patients suffering from pancreas pathologies must ensure accurate diagnosing allowing to choose adequate tactics of treatment in proper time.
Choosing of diagnostic method depends on its availability, informativity, possibility of graphic registration of acquired data, safety and affordability. At the present moment neither method of clinical and hardware examination cannot solve problems of modern diagnostics of pancreas pathologies independently.
Leading position in detection of pancreas pathologies is taken by radiological methods, although their accuracy is far from perfect.
Recently appeared NLS-diagnostics method allows to acquire sufficiently accurate information about parenchyma’s and pancreatic ducts system’s condition. But until now two-dimensional NLS-graphy leaves unsolved certain issues related to spatial relations of examined structures and character of affection; in theory this issues may be addressed by three-dimensional NLS-graphy with spectral-entropic analysis (SEA) of tissues.
So, one of the most prospective directions of NLS-diagnostics development is a method of three-dimensional reconstruction of NLS-image, allowing to visualize projections hidden for two-dimensional scanning and to carry out anatomical reconstruction of researched area. This method allows to see any projection of acquired image, select separate parts of it and operate the data interactively using rotation and scaling of researched structures.
The objective of the study is to evaluate informativity of three-dimensional reconstruction of NLS-image in diagnostics of chronic pseudo-tumor-like pancreatitis.
Material and methods of the study
We carried out a retrospective analysis of clinical records of 328 patients admitted to the Erasme academic hospital in 2010-2011. The patients suffered from a hepatopancreatobiliary system organs pathologies complicated by a biliary obstruction; these patients formed a main group. The first (control) group consisted of 30 patients treated in a hospital who had no pathologies of a gastrointestinal tract and a hepatopancreatobiliary system; the second group consisted of 30 patients with diagnosed chronic pseudo-tumor-like pancreatitis.
Patients’ parameters are shown in the Table 1. Among patients of this group male patients prevailed, apparently it is related to peculiarities of male consumatory behavior. Patients complained about chronic long-term disease of gastrointestinal tract organs: pain in epigastrium and dyspepsia (100%), general weakness and loss of appetite (93.3%), loss of weight (76.6%). Continuance of symptoms ranged from several months to 10 years. All patients of the second group had gastrointestinal tract organs diseases and preceding surgical interventions in their medical history. In the second group there were many cases of pancreatic secretory and excretory dysfunction. Pancreatic diabetes was diagnosed in 20% of patients, hyperglycemia episodes (glucose level above 6.7 mmol/l) were detected in almost half of all patients (43.3%). Signs of chronic pancreatitis complications (increasing of α-amylase) at the moment of admission were detected in every fifth patient.
Table 1. Parameters of studied patients
|
Parameters |
1st group (n = 30) |
2nd group (n = 30) |
|
Age, years |
42-72 |
29-89 |
|
Sex (male/female) |
1/1 |
3/2 |
|
Stomach and duodenum pathologies (absolute and relative (%) amount) |
– |
30 (100) |
|
Pancreatic diabetes (absolute and relative (%) amount) |
– |
6 (20) |
|
Chronic viral hepatitis (B or C) (absolute and relative (%) amount) |
– |
2 (6.7) |
|
Surgical interventions because tumors in other organs in medical history (absolute and relative (%) amount) |
– |
6 (20) |
|
Cholecystectomy in medical history (absolute and relative (%) amount) |
– |
8 (26.7) |
|
Surgical interventions into distal part of common bile duct in medical history (absolute and relative (%) amount) |
– |
4 (13.4) |
|
Surgical interventions into stomach and duodenum in medical history (absolute and relative (%) amount) |
– |
4 (13.4) |
|
Hyperbilirubinemia symptoms at admission |
– |
12 (40) |
|
Hyperamylasemia symptoms at admission |
– |
6 (20) |
At the initial stage all admitted patients were subjected to the usual two-dimensional NLS-study of a hepatobiliary system’s organs with evaluation of bile-excretory ducts, the major duodenal papilla and the head of pancreas. Further on we applied methods of three-dimensional reconstruction of a NLS-image with the SEA and other hardware and laboratory methods and techniques in accordance with medical and financial standards for this nosological form of a disease.
NLS-studies were carried out using the “Metatron”-4025 system (the IPP, Russia) equipped with a high-frequency trigger sensor of 4.9 GHz frequency.
To acquire a high-quality statistically relevant three-dimensional image we used various modes of reconstruction.
– Multi-plane volumetric reconstruction (4D-Tissue) of NLS-image mode; it renders a cube, a cross-cut image of which can be viewed in any of three orthographical projections. Thanks to this a multi-plane three-dimensional image of any anatomical structure is created at any plane section.
– Multidimensional representation of color-coded NLS-data mode; it creates an image of organ’s vessels and tissues surface in various colors. It is used to clarify spatial position of vessels and tissues of researched area.
If focal changes of the pancreas head of bile-excretory duct walls were found, we used adjustable transparency and selection of separate tissues mode (DeepVision), which allows to study deep structures, normally hidden by other tissues, segmentation (FastVision) and rotation of acquired three-dimensional model.
The results of the three-dimensional NLS-graphy were compared with data acquired with laboratory studies of the patients, results of standard ultrasound in two-dimensional mode, fibrogastroduodenoscopy, multi-layer spiral CT (MSCT), magnetic-resonance cholengiography (MRCG), endoscopic retrograde cholangiopancreatography (ERCPG) and intraoperative findings (table 2).
The results of a spectral-entropic analysis were compared with cytological/histological studies data acquired with a needle biopsy and during surgical interventions. At the same time we received no evidence of a malignant affection of a pancreas in all cases.
Statistical analysis of acquired data was carried out by standard methods. Quantitative signs are represented in form of a median, 2.5-97.5 percentile, of minimum (min) and maximum (max) values. Differences were considered to be relevant at р ≤ 0.05.Also we calculated response characteristics, specificity and accuracy of various methods of medical visualization (two-dimensional and three-dimensional NLS-graphy, MSCT) in diagnostics of chronic pseudo-tumor-like pancreatitis.
Table 2. Parameters of hardware studies.
|
Parameters |
1st group (n = 30) |
2nd group (n = 30) |
|
Two-dimensional NLS-graphy (absolute and relative (%) amount) |
30 (100) |
30 (100) |
|
Three-dimensional NLS-graphy (absolute and relative (%) amount) |
30 (100) |
30 (100) |
|
Fibrogastroduodenoscopy (absolute and relative (%) amount) |
30 (100) |
30 (100) |
|
MSCT (absolute and relative (%) amount) |
18 (60) |
30 (100) |
|
MRCG (absolute and relative (%) amount) |
– |
2 (6.7) |
|
ERCPG (absolute and relative (%) amount) |
– |
4 (13.3) |
Results of the study and discussion
Radiodiagnosing of any volumetric neoplasm of pancreas is based on detection of a focal affection, partial or complete increasing of its size, changing of its form and surrounding tissues and organs. Diagnostics of chronic pseudo-tumor-like pancreatitis, in a form of a local affection of any part of pancreas along with its increasing is a very difficult task. Chronic inflammatory process, fibrosis and calcification in a parenchyma are presented in form of separate areas of increased chromogenity. Considerable dilation of major pancreatic duct is detected quite often.
During aggravation of an inflammatory process chromogenity of detected neoplasms may increase greatly (up to 5-6 points on Fleindler’s scale). Depending on size of affected areas, one may detect both micro- and macrofocal affection of parenchyma.
If a process is localized in the head of pancreas its increasing and form roughness may be revealed. In this case one may observe squeezing of a distal part of a common bile duct leading to its dilation above the obstruction point.
Long-termed clinical course of the second group patients’ diseases, in comparison with the control group, resulted in more frequent diagnosing of liver parenchyma structure changes (heterogeneity of echostructure, increasing of chromogenity).
Co-occurring concretion of gall-bladder were detected in 30% of the second group patients (excluding patients subjected to cholecystectomy earlier). Concretion of a common bile duct was detected in 7 patients (23.3%).
The size of a gall bladder was statistically equal in both studied groups. Maybe it was related to the fact that in almost a half of patients a cholelithiasis with chronic inflammation and fibrosis of a gall bladder walls was present.
Because of the fact that chronic inflammatory process was more often localized in a head of pancreas and caused squeezing of intrapancreatic part of common bile duct, in all patients of the second group we detected signs of biliary obstruction of various stages. In patients subjected to ERCPG we detected thickened uneven walls of common bile duct in distal part and aerobilia.
Presence of pseudo-tumor-like pancreatitis led to reliable increasing of pancreas head size (indirect symptom) in comparison with control group. Because of a prolonged clinical course of the disease, much more often we detected uneven form and changing of a pancreas parenchyma’s structure (heterogeneity) (86.7%). Diffuse-heterogeneous increasing of parenchyma’s chromogenity (5-6 points on Fleindler’s scale) was found in 73.3% of patients. In 26.7% of patients we detected moderate chromogenity (3-4 points) of pancreas parenchyma. Increasing of major pancreatic duct was detected in a half of the patients. In case of significant dilation of major pancreatic duct a thickening of its walls was found.
Against the background of pancreas changed parenchyma, in all patients (as a rule in the head and the body of the organ) neoplasms of high chromogeneity, diffuse heterogenic structure, uneven round or oval form, of 0.8 – 3.5 cm size were visualized. When these neoplasms were located near the edge of pancreas, a deformation of the gland’s form was detected (but without solution of capsule’s continuity). Numerous small diffuse-located hyperchromogenic areas (fibrosis and calcinosis) were found in these neoplasms. We faced additional difficulties when inflammation spread to parapancreatic cellular tissue, which may imitate tumorous invasion. Differential diagnostics with blast processes was carried out using the SEA. These neoplasms were visualized in a pancreas within 2 months, gradually decreasing in size.
When we applied three-dimensional NLS-ultramicroscanning of bloodstream to examine patients suffering from pseudo-tumor-like pancreatitis, in detected lumps we found signs of thrombosis without violation of angioarchitecture. This symptom was found in all (100%) patients of the second group. In all groups we found no signs of portal vein thrombosis.

Pic.1. 2D NLS-scanning. A calcification in pancreas head projection.
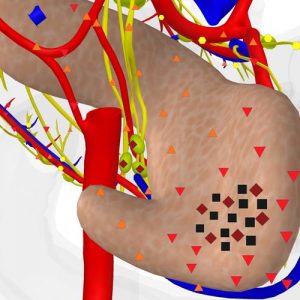
Pic.2. 3D NLS-graphy. Multiplane 3D rendering mode. Pseudo-tumor-like pancreatitis. Hypochromogenic neoplasm of 2×1.5 cm sixe in pancreas head.
Application of superficial multidimensional reconstruction with adjustable transparency improved greatly quality of visualization of both internal structures of detected neoplasms and their contours. Multi-plane and multidimensional reconstruction allowed to detect more precisely localization of neoplasms in a pancreas and their edges. Using of various modes of three-dimensional reconstruction allowed to detect clear division between this neoplasm and parenchyma of pancreas in 28 patients (93.3%).
Affection of regional lymph nodes (at superior and anterior edge of pancreas head and along hepatoduodenal ligament) was registered in 70% of patients of this group. As a rule lymph nodes were characterized by slightly increased chromogeneity (4-5 points at Fleindler’s scale) with distinct contours. It is very difficult to tell the difference between mentioned changes of lymph nodes and tumorous affection by usual two-dimensional NLS-study. We were able to judge about character of changes in lymph nodes only by analyzing of the SEA data, which was confirmed by biopsy.
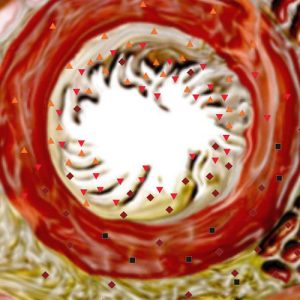
Pic.3. NLS-ultramicroscanning. Pancreatic duct walls. Pseudo-tumor-like pancreatitis with squeezing of the duct distal part.
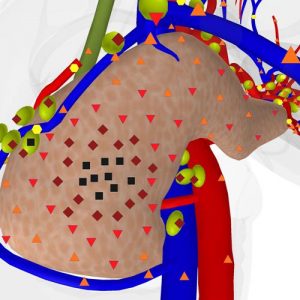
Pic.4 3D NLS-graphy. Pseudo-tumor-like pancreatitis. Multiplane 3D rendering mode. Affection of lymph nodes in pancreas head area.
Undular clinical course of pancreas chronic disease, often resulting in biliary obstruction, was typical for major part of the second group patients. Obstruction of extrahepatic bile ducts leads to increasing of pressure in bile tract and hypertension in intrahepatic bile ducts. Intrahepatic cholestasis is added to extrahepatic cholestasis and thus the process becomes a combined one. So, hyperbilirubinemia (total bilirubin more than 25 mcM/l) was diagnosed in 40% of patients of this group (Table 3). Due to long clinical history of the disease in every fourth patient anemia was found. Increasing of blood sedimentation rate was found in every third patient and was related to aggravation of the inflammation. In some patients we found slight increasing of tumor markers levels, which required further scheduled examination of hepatopancreobiliary system’s organs in order to exclude development of tumorous process.
Table 3. Laboratory analysis of blood
|
Parameters |
1st group (n = 30) |
2nd group (n = 30) |
|
Total bilirubin, mcM/l |
11,9 (4,6-19,2) (3,9-20,6) |
16,9 (10,0-105,8) (6,8-320,0) |
|
Conjugated bilirubin, mcM/l |
2,1 (2,0-3,6) (1,7-3,8) |
5,5 (2,5-72,1) (1,5-222,0) |
|
Unconjugated bilirubin, mcM/l |
10,5 (3,7-16,1) (2,9-17,5) |
10,1 (7,0-42,9) (5,5-98,0) |
|
BUN, M/l |
4,90 (3,70-6,60) (3,00-7,50) |
5,34 (3,66-7,02) (2,43-7,69) |
|
Creatinine, mcM/l |
92,0 (72,0-106,0) (55,0-112,0) |
67,8 (63,6-82,0) (61,0-103,9) |
|
Glucose, M/l |
5,2 (4,7-6,0) (4,1-6,1) |
5,7 (4,5-6,9) (4,1-8,4) |
|
Alanine aminotransferase, mcM/l |
29,8 (11,5-39,8) (10,3-48,9) |
40,9 (15,9-98,0) (11,5-211,8) |
|
Aspartate aminotransferase, mcM/l |
32,6 (15,7-38,1) (14,2-43,8) |
40,8 (28,4-105,1) (20,6-183,1) |
|
Alkaline phosphatase, IU/l |
86 (51-125) (44-156) |
308 (208-934) (135-2582) |
|
Amylase, U/l |
46 (24-71) (21-79) |
54 (29-109) (13-138) |
|
Ca-19-9, U/l (normal value – up to 37 units per ml) |
_
|
14,0 (8,7-47,8) (2,5-262,0) |
|
Ca-125 U/l (normal value – up to 35 units per ml) |
_
|
23,8 (5,2-61,9) (2,3-92,7) |
|
Ca-153 U/l (normal value – up to 38 units per ml) |
_
|
22,1 (12,8-41,7) (9,2-90,7) |
|
Carcinoembryonal antigen, ng/ml (normal value – up to 7 ng/ml)( 2.26–8.40) |
_
|
2,95 (2,26-8,40) (1,19-18,73) |
A need in application of MSCT and ERCPG appears when it is not possible to visualize clearly some areas of a pancreas by the NLS-study or when there is an assumption of volumetric processes in a pancreas.
MSCT was applied to all 30 patients (100%) in order to specify a character of pancreatic disease. According to acquired data, in case of absence of pancreas size increasing, MSCT has less informativity in comparison with three-dimensional reconstruction, because it does not provide clear information about changes in its parenchyma, when radiologic densitometric density of pancreas tissues is close to normal values.
MSCT gives a possibility to diagnose on a stage of pancreatitis aggravation: at calcinosis, forming of pseudocysts, affection of surrounding organs or pancreas parenchyma atrophy. This method allows to evaluate affection of soft tissues beyond pancreas and surrounding structures in order to evaluate prevalence of the process and inflammatory response of parapancreatic tissue and retroperitoneal space. But sometimes fibrosis and inflammatory changes may imitate tumorous invasion.
A disadvantage of this diagnostic method is its high costs. Another disadvantage is a strict binding of acquired images to transverse plane.
MRCG was administered to 2 patients only because of common bile duct distal part stenosis and it gave no additional information about the reasons of stenosis development. Main disadvantages of MRCG are: high cost of a research, using of contrast, radiologic stress and impossibility of a scanner transportation to a patient.
Informativity of two-dimensional and three-dimensional NLS-graphy and MSCT in revealing of chronic pseudo-tumor-like pancreatitis is shown in the table 4.
Table 4. Informativity of various diagnostic methods (%)in revealing of chronic pseudo-tumor-like pancreatitis.
|
Diagnostic methods and techniques |
Response |
Specificity |
Accuracy |
|
Two-dimensional NLS-graphy |
63,3 |
81,5 |
78,1 |
|
Three-dimensional NLS-graphy |
93,3 |
99,0 |
98,5 |
|
MSCT |
83,3 |
96,3 |
95,0 |
ERCPG allows to find changes in a duct system (dilation, roughness, stenosis), localize an obstruction, detect intraductal calcification and protein plugs. Extent of found by ERCPG changes may not correspond to intensity of functional and structural changes in a pancreas. The disadvantage of this method is impossibility to evaluate changes of pancreas parenchyma directly.
All 4 applications of ERCPG were scheduled and carried out for treatment purposes (lythoextraction or papillosphincterotomy at stenosis of major duodenal papilla). No complications were registered after this procedure.
Various types of surgical interventions on organs of hepatopancreatobiliary system were performed on 7 patients (23.3%) of the second group. The majority of surgical interventions were diagnostic ones (4 operations – 57.1%). But in the last 18 months (after mastering of three-dimensional NLS-graphy and developing of examination and monitoring algorithm) this type of surgical interventions was never repeated. In three cases patients refused to be subjected to surgery. In the rest of cases operations were not recommended because of compensated state of patients. As we noted before, morphological study was administered to 30 patients (100%) of the second group.
After NLS-study of 328 patients admitted to the hospital with hepatopancreatobiliary system organs pathologies complicated by biliary obstruction, we found no statistically reliable difference between two-dimensional and three-dimensional NLS-graphy in revealing of indirect symptoms of biliary obstruction: changes of bile-excretory ducts and gall bladder, changes in liver typical for cholestasis, dilation of major pancreatic duct.
Application of various modes of three-dimensional NLS-graphy allowed to acquire data showing 1.8 times improving in revealing of biliary obstruction symptoms.
Conclusion
Three-dimensional image rendering improves visualization in revealing of pancreas structure changes. Superficial multidimensional image reconstruction with adjustable transparency feature improves quality of visualization of both internal structure of revealed neoplasm and its shape and contours. In case of duct system (common bile duct and major pancreatic duct) dilation this mode allows to distinguish external contour of duct wall from neighboring tissues and internal surface of wall from a cavity content, to monitor structure of duct wall in the investigated area.
Multi-plane multidimensional reconstruction of an image with segmentation feature allows to localize and define size of a neoplasm in pancreas parenchyma and to evaluate borders with surrounding tissues, ducts and vessels.
Multi-plane multidimensional reconstruction of an image with color-coded methods allows to carry out three-dimensional reconstruction of tissues and vessels that reveals convincing signs of affection.
Thus application of three-dimensional NLS-graphy with SEA allows to:
– carry out more precise differential diagnostics between benign and malignant nature of detected pancreatic neoplasms;
– define clearly indications for extended diagnostics (evaluation of spectral similarity with oncological markers) in order to exclude tumorous affection of pancreas;
– exclude in some cases duplicating radiologic methods (MSCT and MRCG), which optimizes diagnostic algorithm of patients examination;
– decrease a risk of complications development, related to using of invasive methods of diagnostics (ERCPG, needle biopsy);
– choose treatment tactics in proper time;
– ensure dynamic monitoring in a diagnostic department for patients from pancreas tumor development risk group.
In order to exclude a possibility of tumorous process development in pancreas all patients with diagnosed chronic pseudo-tumor-like pancreatitis and moderate increasing of tumor markers level are recommended for dynamic monitoring in a diagnostic department.
References
1. Cameron J.L. Pancreatic Cancer: Atlas of Clinical Oncology. Hamilton, London: BC Decker Inc., 2001. 457 p.
2. Sabiston Textbook of Surgery: the Biological Basis of Modern Surgical Practice. 16th ed. / Ed. By Townsend C.M. Jr. Philadelphia: W.B. Saunders Company, 2001. 1076 p.
3. Koito K., Namieno T., Nagakawa T. et al. Pancreas: imaging diagnosis with color/power Doppler ultrasonography, endoscopic ultrasonography, and intraductal ultrasonography // Eur. J. Radiol. 2001. V.38. № 2. P. 94–104.
4. Campani R., Bottinelli O., Calliada F., Coscia D. The latest in ultrasound: threedimensional imaging. Part II // Eur. J. Radiol. 1998. V. 27. Suppl. 2. P. S183–S187.
5. Rohling R.N., Gee A.N., Berman L. Automatic registration of 3D ultrasound images // Ultrasound Med. Biol. 1998. V. 24. № 6. P. 841–854.
6. Sanches J.M., Marques J.S. A multiscale algorithm for threedimensional freehand ultrasound // Ultrasound Med. Biol. 2002. V. 28. № 8. Р.1029–1040.
7. Masci E., Mariani A., Curioni S., Testoni P.A. Risk factors for pancreatitis following endoscopic retrograde cholangiopancreatography: a metaanalysis //Endoscopy. 2003. V. 35. № 10. P. 830–834.
8. V.I. Nesterov. Computer nonlinear diagnostics. Collection of scientific papers of the Institute of Practical Psychophysics “Current problems of NLS-diagnostics”. Tome 1. Moscow. Katalog, 2006, p. 5-6.
9. S.P. Tokar, A.S. Davydova, T.L. Guseva, V.I. Gusarov, Z.F. Khabibullina, L.S. Pugacheva. Non-linear computer diagnostics and pathology of hepatopancreaticoduodenal area. Collection of scientific papers of the Institute of Practical Psychophysics “Current problems of NLS-diagnostics”. Tome 1. Moscow. Katalog, 2006, p. 77-88