A.Y. Shvack, T.G. Kuznetsova, V.I. Nesterova, G.A. Lopukhov
Clinic of postgraduate education department of the Omsk state medical academy
In order to evaluate informativity of a three-dimensional NLS-graphy in diagnostics of a cholangiocarcinoma, we carried out a retrospective analysis of clinical records of patients admitted to the Clinic of postgraduate education department of the Omsk state medical academy in 2009-2011. The first (control) group consisted of 30 patients treated in a hospital who had no pathologies of a gastrointestinal tract; the second group consisted of 23 patients with diagnosed benign stenosis of major duodenal papilla of the 3rd stage, complicated by cholangitis and choledocholithiasis; the third group – 21 patient with tumorous affection of hepatopancreoduodenal area organs (tumors of common bile duct, major duodenal papilla and head of pancreas); the fourth group – 12 patients with cholangiocarcinoma. We carried out a comparative analysis of a two-dimensional and a three-dimensional NLS-graphy, CT, endoscopic retrograde cholangiopancreatography.
Introduction
Intrahepatic cholangiocarcinoma is diagnosed in 7-35% of all malignant hepatic neoplasms cases. Early detection of this pathology is one of the most difficult tasks in diagnostics in hepatology, because the tumor often develops against the background of chronic diseases of liver and bile-excretory ducts and disguised by symptoms of these diseases.
In recent years periodicity of cholangiocarcinoma detection increased. It is explained by introduction of modern methods of visualization, which allow to specify localization and prevalence of tumorous process more accurately. The high point of disease incidence is at the age of 50-70. The incidence of the disease in men and women is almost equal.
The main syndromes accompanying the disease are obstructive jaundice and cholestasis, which decrease greatly parenchyma’s regeneration ability. At the late stages of the disease suppurative cholangitis appears, which oftimes becomes a cause of death of a patient.
Cholangiocarcinoma has adenous structure and originates from intrahepatic bile ducts epithelium, containing keratin, which explains its density. A tumor may develop at any level of biliary tree and spread into a liver. Due to the fact that a tumor is characterized by slow infiltrating growth inside or along duct wall, it does not form clearly visualized volumetric neoplasm and has no clear borders. When a tumor squeezes bile ducts, a biliary hypertension of various intensity and dilation of superjacent parts of biliary tract (depending on a tumor spread) appear. Below the obstruction point a diameter of common bile dust and size of gall bladder decrease.
It is not always possible to reveal a reason of cholestasis analyzing clinical symptoms and biochemical indices only, especially in patients with relatively short and low hyperbilirubinemia. It is also important that the majority of patients suffering from this pathology is elderly people and is admitted to a hospital’s surgery departments with already developed complications.
The only efficient method of cholangiocellular carcinoma treatment is a surgical intervention, which emphasizes the importance of well-timed examination to reveal “lesser” tumors. In patients with small tumors 5-years survival rate reaches 85%. The main factor determining resectability of a tumor is functional possibilities of remaining part of a liver.
Methods of the highest importance for primary diagnostics of bile-excretory dusts pathologies are non-invasive methods of research (ultrasound scanning, computed tomography and magnetic resonance imaging). But these methods cannot clearly detect a localization of a focal process and its character. Basing of acquired data therapists decide about the more accurate method of invasive diagnostics: endoscopic retrograde cholangiopancreatography (ERCPG), percutaneous transhepatic cholangiography (PTCG), and in some cases – angiographic study and liver biopsy. Choosing of a method is determined by its availability, information value, safety and affordability.
Recently appeared method of non-linear diagnostics (NLS) may now become the most available method for primary diagnostics of abdominal cavity diseases. One of the most-prospective trends of NLS-diagnostics is three-dimensional NLS-graphy, which has certain technical and practical advantages in visualization of anatomic and pathological structures over other methods of hardware visualization. Data acquired after computer processing can manipulated, a plane of three-dimensional model cross-cut can be adjusted, thus allowing to investigate organs images in various projections.
The objective of the present study is to evaluate possibilities of three-dimensional NLS-study in diagnostics of cholangiocarcinoma.
Material and methods of the study
We carried out a retrospective analysis of clinical records of patients admitted to the Clinic of postgraduate education department of the Omsk state medical academy in 2009-2011. The first (control) group consisted of 30 patients treated in a hospital who had no pathologies of a gastrointestinal tract; the second group consisted of 23 patients with diagnosed benign stenosis of major duodenal papilla of the 3rd stage, complicated by cholangitis and choledocholithiasis; the third group – 21 patient with tumorous affection of hepatopancreoduodenal area organs (tumors of common bile duct, major duodenal papilla and head of pancreas); the fourth group – 12 patients with cholangiocellular carcinoma.
The majority of patients were of middle and old ages. Accompanying pathology of gastro-intestinal tract organs was in clinical history of the major part of patients of the 2-4 groups. Concrements in gall bladder at the moment of the study were in 91.3% of patients of the second group, 57.1% patients of the third group and 50% – of the fourth. Biliary obstruction symptoms continuance ranged from several days till 4 months. 4 patients of the second group (17.4%) were earlier subjected to various types of operative interventions on distal parts of a common bile duct (papillosphincterotomy, pancreaticoduodenal resection).
Most often cholangiocarcinoma developed in patients with affection of hepatic parenchyma. In 58.3% of patients of the fourth group we detected chronic hepatitis B and C, which corresponds to information given in references. In HBsAg-positive patients risk of liver cancer development is 30 times higher. Also in 25% of patients of this group an oncologic pathology of other organs was registered in clinical history.
All admitted patients at the first stage were subjected to ultrasound investigation of hepatopancreobiliary system organs with mandatory study of bile-excretory ducts, major duodenal papilla and head of a pancreas. Further on, in order to specify nosological form of a disease, we used other hardware and laboratory methods in correspondence with medical and financial standards and the three-dimensional NLS-graphy with spectral-entropic analysis (SEA), which allowed to define a character of volumetric neoplasm in a liver and bile ducts according to a spectral similarity with etalon processes.
NLS-researches were carried out using “Metatron”-4025 systems (the IPP, Russia) equipped with high-frequency trigger sensor (4.9 GHz), a unit of continuous spiral scanning and a feature of three-dimensional rendering. Acquired data was processed with specialized software “Metapathia GR Clinical”. For detailed evaluation of revealed changes we used modes of ultramicroscanning, rotation, segmentation and multi-plane imaging.
Results of three-dimensional NLS-graphy were compared to the data acquired during laboratory tests, ultrasound investigation, computed tomography, ERCPG, fibrogastroduodenoscopy and surgery interventions. SEA results were compared with results of cytological and histological studies.
According to SEA results in the third group there were 7 patients with adenosquamous carcinoma (cancer), 1 with non-differentiated (anaplastic) carcinoma and in 13 patients – adenocarcinoma. In all 12 patients of the fourth group we diagnosed intrahepatic cholangiocarcinoma. SEA results were confirmed by cytological and histological studies results in 98.3% of cases.
Statistical analysis of acquired data was carried out by standard methods. Quantitative data is represented in form of a median, 2.5-97.5 percentile, of minimum and maximum values. Differences were considered to be relevant at р ≤ 0.05.
Results of the study and discussion
Nowadays the symptoms of intense intra- and extrahepatic cholangiectasis are well known: presence of volumetric intra- and periductal neoplasms obstructing patency of bile-excretory ducts; presence of dilated intra- and extrahepatic bile ducts with superjacent obstruction point, etc. But still we have no diagnostically significant criteria of biliary obstruction development reasons at the early stages, before intense clinical symptoms of jaundice appear.
Due to increased number of surgery interventions on bile-excretory ducts, number of late post-surgery complications increased. One of such complications is benign strictures of bile ducts. In 90% of cases secondary strictures of major duodenal papilla are found, the reasons of which are: constrictor fibrosis, caused by concrements migration; consequences of abdominal, operational or endoscopic trauma; duodenum ulcer; ray therapy; pancreatitis, recurrent cholangitis and other non-specific inflammatory processes, affecting excretory function of bile-excretory ducts.
Significant difficulties in differential diagnostics of intrahepatic bile ducts dilation reason appear in patients with acute or chronic cholangitis. Quite often cholangitis develop in patients suffering from choledocholithiasis. According to references, in 5-10% of patients cholecystectomy with revision of common bile duct cannot remove all concrements. Most often stones in intrahepatic bile ducts remain intact. Bile stagnation leads to its contamination with intestinal microflora. Common bile duct is dilated, desquamation and cankering of mucous tunic are registered. When cholangitis spreads to intrahepatic bile ducts, liver abscesses may be formed. Continuous stand of a concrement leads concentric cicatrization of bile-excretory ducts, resulting in development of secondary sclerosing cholangitis and biliary cirrhosis.
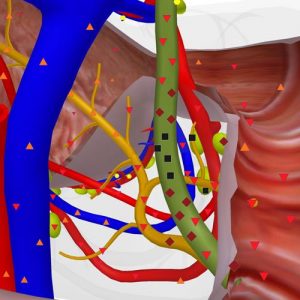
Pic.1. Patient F., 60 years old. Tumorous affection of common bile duct. Three-dimensional NLS-graphy in a mode of multi-plane multidimensional rendering of a image
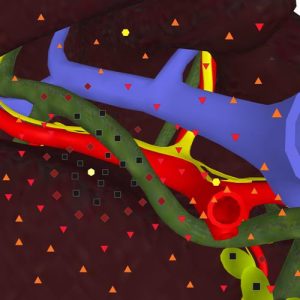
Pic.2. Patient E., 58 years old. Segmented intestine cancer metastasis into a liver with growing into left lobe bile duct. Three-dimensional NLS-graphy.
In majority of patients of the second group (82.6%) we noted presence of accompanying choledocholithiasis. Adequate setting of a patient and proper methodological approach may ensure diagnosing of common bile duct distal part dilation even at scheduled ultrasound check-up. 3D NLS-diagnostics method allowed to visualize more accurately area of affection in common bile duct and formulate indications for ERCPG. When this pathology was confirmed, we carried out correction using endoscopic papillosphincterotomy. If it was not possible, a hepaticojejunostomy was applied by surgical way.
Normal values of oncomarkers and a possibility to monitor patients in dynamics after active conservative or surgical therapy can help in proper diagnosing.
Tumors of major duodenal papilla, distal parts of common bile duct and pancreas head due to tumorous invasion, circular squeezing and growing into a duct can lead to an obstruction (the third group of patients). At the same time the following symptoms of biliary obstruction are revealed: dilation of proximal parts of bile ducts; enlarging of gall bladder; development of hepatic changes typical for cholestasis. At accompanying obstruction of a major pancreatic duct directly at the point of its transition into a capsule, a dilation of the duct superjacent to a point of the obstruction is detected.
A direct sign of a major duodenal papilla tumor is a volumetric neoplasm in its projection. At growing of a neoplasm into duodenum we detected constriction and tortuosity of a distal part of a common bile duct and severe damage of a papilla walls, chromogeneity of which was significantly heightened during NLS-research (6 points at the Fleindler’s scale). If a tumor grows towards a common bile duct, in its dilated opening in major duodenal papilla projection, NLS-study detected a neoplasm of varied chromogeneity, which obstructed the duct. Especially clearly advantages of three-dimensional NLS-graphy in detection of tumors in this area in comparison with ultrasound are seen if major duodenal papilla tumor’s size is less than 5 mm.
Direct signs of common bile duct tumorous affection were local thickening of duct wall with disorders of layer structure and hyperchromogenic neoplasm in duct opening. Visualization of damaged wall improved greatly after three-dimensional NLS-ultramicroscanning was applied.
A significant NLS-sign of pancreas head tumor is a direct visualization of a volumetric neoplasm – a solid nidus (of increased chromogeneity, as a rule) or hypochromogenic cystic and solid neoplasm with bordering line between a tumor and surrounding tissues. If pancreas head tumor causes obstruction of two duct systems, a common bile duct and a major pancreatic duct may be visualized as neighboring roundish hypochromogenic structures. If a tumor is located close to vessels, signs of extravasal compression and walls invasion are visualized. A fundamental importance for proper diagnosing belongs to NLS-ultramicroscanning with SEA for sure. The best results of three-dimensional reconstruction of NLS-image was achieved in diagnostics of “lesser” tumors of pancreas head (less than 5 mm). Using of three-dimensional NLS-ultramicroscanning allows to define more precisely size of tumors and their relation to surrounding vessels and bile ducts, extent of surrounding tissues invasion.
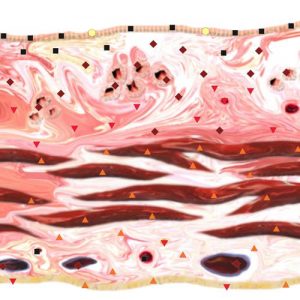
Pic.3. Patient B., 65 years old. NLS-ultramicroscanning. Cholangiocarcinoma located in major hepatic duct.
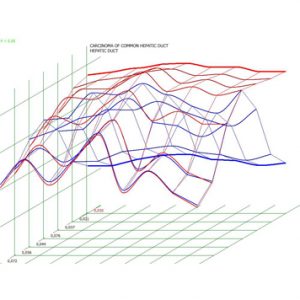
Pic.4. Patient V., 68 years old. Spectral-entropic analysis. Cholangiocarcinoma (D = 0,030)
A dilation of intrahepatic ducts may be detected in patients with metastatic lesions of a liver. Revealing of volumetric neoplasms located near the dilated duct may help in diagnosing of the dilation reasons.
As we noted before, in majority of cases cholangiocarcinoma does not form clearly defined volumetric formation, it has no clear borders and its chromogeneity is only slightly different from healthy tissue of a liver. Often only results of SEA show presence of a tumor.
If a process is generalized (25%) metastases into regional lymph nodes, located in projection of portal fissure, hepatopancreoduodenal ligament and pancreas are visualized.
Using of three-dimensional NLS-graphy allows to visualize more accurately a tumor itself, trace spreading of a tumor along bile duct and through its walls; application of SEA helps to differentiate metastatic and inflammatory character of surrounding tissues affection. Sometimes annular stricture and occlusion of intra- and extrahepatic bile-excretory ducts is detected. At development of accompanying cholangitis, affection of ducts walls is visualized clearly.
Size of detected by NLS-ultramicroscanning tumors, according to our data, is from 2.5 mm to 5 mm. The minimal detected cholangiocarcinoma was of 1.5 mm size. Localization of cholangiocarcinoma is shown in Table 1.
Table 1. Localization of cholangiocellular carcinoma (n = 12)
| Localization | Absolute number | Relative number, % |
| Intrahepatic ducts | 2 | 16.7 |
| Common hepatic duct and point of lobar hepatic ducts junction | 5 | 41.7 |
| Diffuse affection of common bile duct | 1 | 8.3 |
| Diffuse affection of biliary tract | 4 | 33.3 |
The fact that in this group of patients severe affection of common bile duct and major pancreatic duct is detected not so often, has a certain meaning for NLS-diagnostics of cholangiocarcinoma.
Table 2 shows indices of information value of various research methods and techniques in revealing of bile ducts affection reasons. Three-dimensional NLS-graphy improves information value of Ultrasound study and CT.
According to references, cholangiocarcinoma invasion into blood vessels is registered rarely. Application of NLS-ultraangiography allows to detect affection of hepatic vessels (tumorous invasion) in majority of cases (83.3%).
It should be noted that any detected local stricture and bile ducts damage must be regarded as malignant, until opposite is proven.
Table 5. informativity (%)of various research methods and techniques in revealing of bile ducts affection reasons.
| Methods and techniques | 2nd group (n = 21) | 3rd group (n = 21) | 4th group (n = 12) |
|
Ultrasound research responce specificity accuracy |
n = 23 86,9 91,7 89,8 |
n = 21 85,7 92,1 89,8 |
n = 12 83,3 95,6 93,1 |
|
Three-dimensional NLS-graphy responce specificity accuracy |
n = 23 98,6 99,1 97,5 |
n = 21 97,2 95,6 96,8 |
n = 12 94,6 99,6 96,8 |
|
Computed tomography responce specificity accuracy |
n = 13 84,6 91,7 89,8 |
n = 21 85,7 92,5 89,6 |
n = 12 99,6 91,9 91,8 |
|
ERCPG responce specificity accuracy |
n = 18 100,0 100,0 100,0 |
n = 12 100,0 100,0 100,0 |
n = 5 100,0 100,0 100,0 |
Application of radiological method of diagnostics (CT and MRI) at cholangiocarcinoma allows to detect a dilation of intra- and extrahepatic bile ducts, but it is much more difficult to visualize tumor itself, density of which is the same as density of liver. The advantage of these diagnostic methods is that they allow to evaluate spreading of tumorous process to surrounding tissues and organs with a greater reliability.
To evaluate level and parameters of bile-excretory ducts stricture, invasive methods of diagnostics are usually used: ERCPG, PTCG, operative cholangiography and biopsy. Still, even after these complex studies, it is not always possible to define a character of an obstruction in common hepatic or common bile ducts.
At development of cholangiocarcinoma, as well as at any other types of obstructive jaundice and accompanying cholangitis, biochemical parameters of blood prove development of cholestatic jaundice. Levels of total and conjugated bilirubin and alkaline phosphatase may be very high. Variation of indices reflects incomplete obstruction or involvement of only one duct. At acute obstruction increased activity of transaminase may be registered. It should be noted that great compensatory abilities of a liver provide preservation of its functioning at the early stages of tumor development. Probably that is why in our study frequency of jaundice and acute pancreatitis revealing in patients with cholangiocarcinoma was less that in patients of the second and the third groups.
According to our data response of СА-19-9 oncomarker level detection was above 80% in patients of the third and the fourth groups. References say that simultaneous detection of СА-19-9 and CEA is more accurate, diagnostic precision in this case reaches 86%.
Thus application of 3D NLS-graphy with SEA allows to: reveal etiological reason of bile ducts affection more accurately; evaluate spreading and intensity of bile ducts damage; evaluate relation of pathological nidi to vessels (branches of portal vein and hepatic artery) and surrounding structures; choose treatment tactics and decide about possibility of radical or nonradical surgical intervention. High resolution at three-dimensional NLS-ultramicroscanning allows to visualize small objects accurately. Application of SEA helps to evaluate morphological character of tumorous affection of tissues and organs, which influences choosing of further treatment.